What is deprescribing?
Let’s start with a couple of definitions!
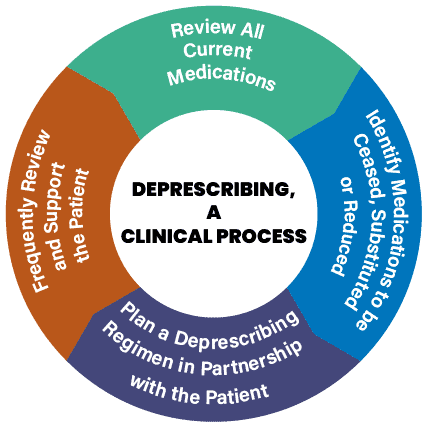
- “Deprescribing is the planned and supervised process of dose reduction or stopping of medication that might be causing harm, or no longer be of benefit. Deprescribing is part of good prescribing – backing off when doses are too high or stopping medications that are no longer needed.”1
- “Reducing polypharmacy should be a priority of clinicians working in nursing homes. Clinicians should evaluate each medication for its utility, taking into consideration such factors as the patient’s life expectancy, the care goals, and the length of time until benefits manifest.”2
Why Deprescribe?
Reducing polypharmacy can help decrease chance of drug interactions, adverse events, falls, improve health outcomes, adherence and patient satisfaction, and decrease healthcare costs.
How can you get started with deprescribing? There are several resources available that can aid with deprescribing:
- ASCP/AMDA/AGS Choosing Wisely Campaign
- AMDA’s Drive to Deprescribe. Optimizing Medication use in PALTC
- Deprescribing Guidelines and Algorithms
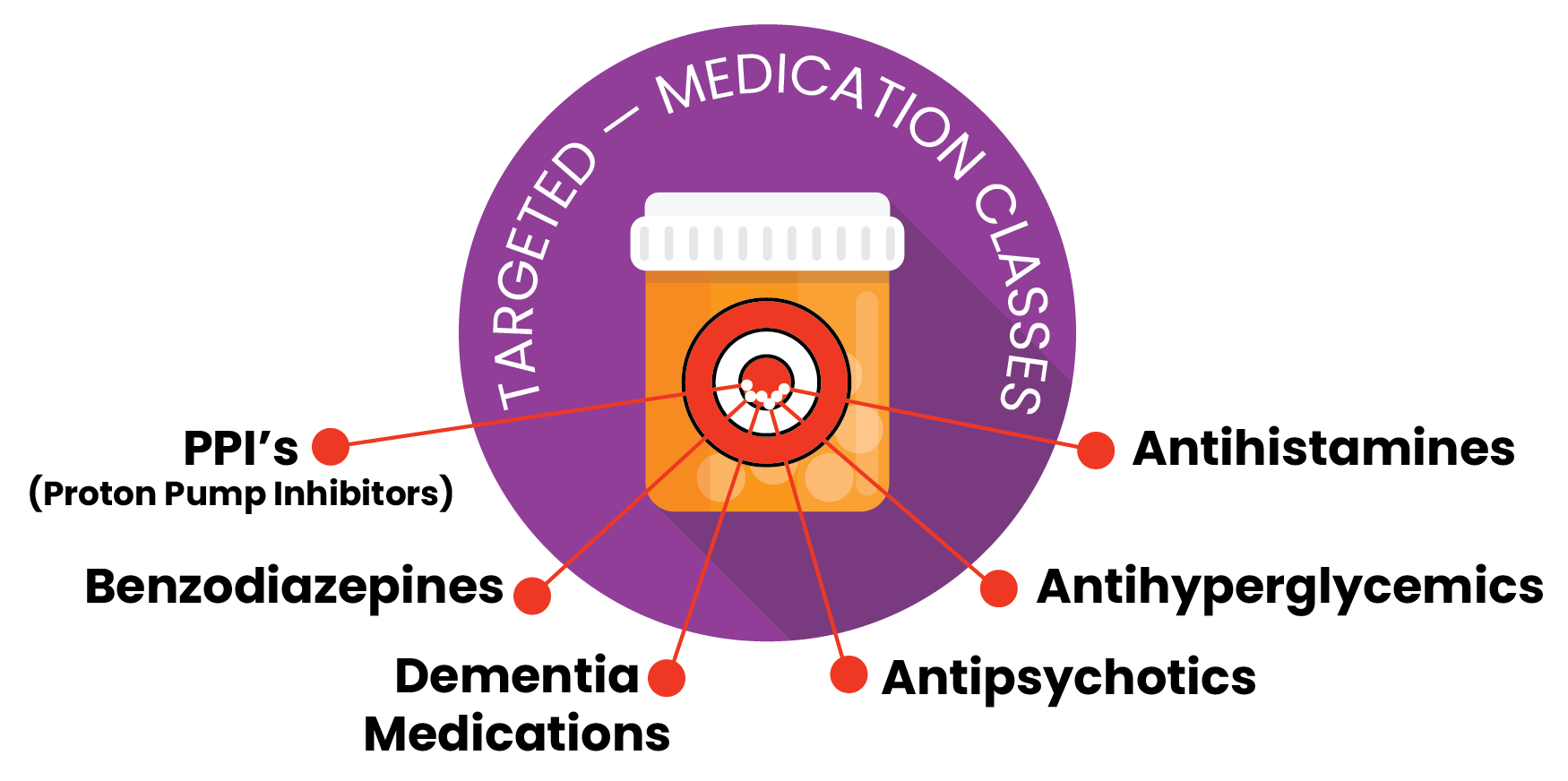
- Tapering algorithms available for PPIs, antihyperglycemics, benzodiazepine and Z-drugs, antipsychotics, dementia medications.
- More algorithms
- Beers Criteria
- STOPP
Some Tips to get started:
Tip #1:
Have you ever heard of the “prescribing cascade?” Perhaps you’ve heard of the snowball effect? The snowball effect is a process that starts from an initial small state of significance and builds upon itself, becoming larger and potentially more serious and dangerous. The prescribing cascade is very similar to the more commonly known snowball effect. It occurs when an adverse drug event (ADE) is misinterpreted as a new medical condition in which another medication is added to address the ADE. You can see how this can become problematic and can lead to the addition of unnecessary medications, which can potentially have serious adverse effects and drug interactions.
- To avoid this from happening, consider a dose reduction or discontinuation of the medication that could be the culprit of the adverse drug event. Consider a more suitable alternative if available.
- Example:
- A calcium channel blocker (CCB) is given for high blood pressure. Edema and constipation develop. A diuretic and stool softener are then prescribed.
- Edema and constipation are common side effects of CCBs. Instead of adding 2 medications to treat the adverse effects, consider an alternative BP lowering agent such as an ACEI or ARB.
Tip #2:
Consider life-expectancy when prescribing new medications or determining whether therapies should be continued or not. Consider time-to-benefit for preventative medications such as statins and bisphosphonates.
Tip #3:
Avoid using 3 or more CNS-active medications as it can increase risk of serious adverse drug events including falls and fractures. Avoid combining opioids with benzodiazepines or gabapentinoids to treat pain. In studies, patients that were prescribed benzodiazepines and opioids experienced 1.66 times more ER visits.
Tip #4:
Avoid highly anticholinergic medications. These medications increased risk of dementia, constipation, blurred vision, urinary retention, and falls.
- Examples include: first generation antihistamines (diphenhydramine), tricyclic antidepressants (amitriptyline, nortriptyline, doxepin), GI antispasmotics (dicyclomine), muscle relaxants (cyclobenzaprine), medications for urinary incontinence (oxybutynin).
- Avoid using anticholinergic medications with cholinesterase inhibitors (antagonistic effects).
Tip #5:
REMEMBER: SOME MEDICATIONS REQUIRE TAPERING WHEN DISCONTINUING TO AVOID WITHDRAWAL OR REBOUND EFFECTS.
Examples include: anticholinergics, antiepileptics, antipsychotics, benzodiazepines, beta blockers,
central alpha-blockers, corticosteroids, H2 receptor antagonists, PPIs.
*** For more specifics on tapering, visit this website for resources ***
PPI’s (Proton Pump Inhibitors):
- Examples include: pantoprazole (Protonix), omeprazole (Prilosec), lansoprazole (Prevacid), esomeprazole (Nexium), etc.
- These medications are commonly used to treat GERD. They are also commonly used to prevent stress ulcers when someone is acutely ill in the hospital. When used for these indications, chronic therapy is usually not indicated. Determine diagnosis and evaluate chronic need.
- Chronic PPI use may be indicated if the patient has Barrett’s esophagus, severe esophagitis, history of bleeding GI ulcer, or is on chronic NSAIDS.
- Why should a lower dose or taper off be considered? In addition to drug interactions, PPI’s can have adverse effects. Adverse effects associated with PPIs can include: headache, diarrhea, nausea, low vitamin B12 and magnesium levels, bone fractures, pneumonia, C. Difficile.
Antihistamines:
- Examples: loratadine (Claritin), cetirizine (Zyrtec), fexofenadine (Allegra), levocetirizine (Xyzal), etc.
- Patients are often placed on antihistamines during allergy season. Sometimes, they remain on them indefinitely. Reevaluate routine need when allergy season is not at it’s peak (October-April). Consider changing to an as needed medication during this time or using a nasal corticosteroid inhaler, which is preferred first line, to manage symptoms.
- Why? Antihistamines are associated with drowsiness, which can increase fall risk. Even the newer antihistamines listed above, can have anticholinergic side effects, although to a much lesser degree than the first-generation antihistamines such as diphenhydramine (Benadryl) or hydroxyzine (Atarax) which should be avoided in the elderly.
Antihyperglycemics:
- Consider deprescribing those that carry a higher risk of hypoglycemia first as LTC patients are at a high risk of hypoglycemia: Examples: sulfonylureas (Glipizide, Glimeperide, Glyburide), insulins, etc.
- Consider patient’s life expectancy, co-morbidities, age, and cognitive impairment when determining A1C goal3,4:
- Healthy (few coexisting chronic illnesses, intact cognitive function): <7.5%
- Complex/intermediate (multiple coexisting chronic illnesses, mild-moderate cognitive impairment): <8%.
- Very complex (LTC or end-stage chronic illnesses, moderate-severe cognitive impairment): Avoid relying on A1C.
- Why? Tight glycemic control can increase fall risk and can worsen cognition. It does not improve overall outcomes but can increase risk of harm.
- In those patients that are well controlled and on low-risk medication regimens, consider decreasing finger sticks to fasting only or twice weekly. This can help improve patient quality of life and compliance.
Antipsychotics:
- Examples: quetiapine (Seroquel), risperidone (Risperdal), aripiprazole (Abilify), haloperidol (Haldol), etc.
- When used for indications such as BPSD (behavioral psychological symptoms of dementia) or insomnia, deprescribing is recommended. Non-pharmacological approaches to manage behavioral symptoms should be implemented and maintained.
- Why deprescribe? Antipsychotics are associated with increased mortality when used in patients with dementia. They are also associated with an increased risk of falls, extrapyramidal symptoms, sedation, weight gain, dizziness, drowsiness, and orthostasis.
- A slow tapering is recommended. Decrease dose by 25-50% every 1-2 weeks.
Benzodiazepines:
- Examples: lorazepam (Ativan), alprazolam (Xanax), clonazepam (Klonopin), diazepam (Valium)
- These types of medications are often used to manage anxiety. SSRI’s are often used in conjunction. Consider tapering off of the benzodiazepine once the SSRI has had time to take effect.
- Avoid use for insomnia. Utilize non-pharmacological therapies to help treat insomnia. Minimize use of caffeine and alcohol.
- Why deprescribe? Benzodiazepines are associated with an increased risk of falls, impaired cognition, drowsiness, sedation, and physical dependence.
- A slow taper is recommended when deprescribing. Reduce dose by 25% every 2 weeks.
Dementia medications5:
- Examples: cholinesterase inhibitors (donepezil (Aricept), rivastigamine (Exelon), galantamine (Razadyne)) and memantine (Namenda)
- These medications are often prescribed to patients with dementia. Consider tapering if:
- Cognition and/or function has significantly worsened.
- No benefit seen.
- Patient has severe end stage dementia (low BIMS score, dependence in most ADL’s, limited life expectancy)
- Why deprescribe? These medications are associated with adverse GI effects, dizziness, headache, insomnia, and falls. They may also cause syncope and bradycardia in rare cases.
- Slow taper by halving the dose every 4 weeks to the lowest dose available, followed by discontinuation.
References:
- What is Deprescribing?
- Maher RL Jr, Hanlon JT, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57-65.
- ADA. Diabetes Care. 2021;44(Suppl.1):S73-84
- ADA. Diabetes Care. 2021;44(Suppl. 1):S168-79
- Deprescibing Recommendations